PRC Research Projects
PRC Projects
The PRC is involved in a variety of national and international multicentre studies. Below you can browse all of them, and find contact information to PI's and study coordinators. Several of the studies are recruiting centres. If your centre is interested in joining, please contact the person stated in the project information site.
MyPath is a 5 year research and innovation project funded by EU Horizon Europe. MyPath is led by Prof. Stein Kaasa from PRC at the Oslo University Hospital’s Department of Oncology, and Marie Fallon, head of the Palliative and Supportive Care group at the University of Edinburgh. This pan-European consortium involving clinicians, researchers, companies, and patient and professional associations will co-create digital patient-centred care pathways and implement them in nine cancer centres in eight European countries. Read more about MyPath here.
Main contact: Stein Kaasa

The 2-year Joint Action on Networks of Expertise (JANE) was initiated in October 2022, financed as part the EU4Health Program. JANE, coordinated by Istituto Nazionale dei Tumori (Italy) and supported by 34 other partners, is endorsed by the EU Commission, and aligns with the EU’s Beating Cancer Plan to improve the diagnosis and treatment of cancer patients across Europe.
The overall JANE goal was to shape seven new Networks of Expertise (NoE) in cancer field, organised as work packages (WP) in the following domains: personalized primary prevention; survivorship; palliative care; omic technologies; hi-tech medical resources; poor-prognosis cancer(s) and young adults with cancer. Five transversal task forces focus on issues important to cancer-related networking in the EU today. More explicitly, the objectives were to prepare everything necessary to launch the new NoEs, and to critically evaluate existing models of current and future EU networking with a view to optimize the functioning of the new NoEs and provide better access to health care services.
Oslo University Hospital has led the WP in Palliative Care. Our proof of concept was based on the Lancet Oncology Commission (Integration of oncology and palliative care: a Lancet Oncology Commission - ScienceDirect) to make PC part of routine cancer care in Europe. Five working groups were established focusing on basic elements to achieve this: defining the content of PC, indicators of PC, implementation, patient-centred pathways, and education/competence. Participants in the WGs come from 10 European countries besides Norway: Denmark, Estonia, Finland, Germany, Italy, Portugal, Romania, Spain, Sweden, and UK. They have provided important contributions and valuable considerations to the WP6 work regarding the diversities in health care organisation in general and oncology/palliative care provision in particular in Europe.
The final JANE report was presented to the EU parliament on Sept. 25th.
The call for a four-year extension of JANE was launched in 2023. The application proved successful, with the official start, November 1, 2024. JANE2 project focuses on sustainability, coordination between NoEs, information-technology infrastructure (including AI), and patient involvement. JANE2 and has 7 clinically oriented WPs and 3 that concern more ad ministrative and overarching themes, e.g. sustainability, evaluation, and dissemination. Read more about JANE2 here: JANE2 - Oslo universitetssykehus HF
Shaping the EU Networks of Expertise on cancer.
Main contacts: Stein Kaasa, Marianne Jensen Hjermstad

Paracetamol with Strong Opioids.
A randomized, double-blind, parallel-group non-inferiority phase III withdrawal trial of paracetamol versus placebo in conjunction with opioids for moderate to severe cancer-related pain.
Ongoing study
Patient inclusion, first patient included in October 2021
Background and study rationale
The World Health Organization's (WHO) three step analgesic ladder has been the standard approach for treating cancer-related pain for more than 30 years. However, this therapy is partly based on tradition and opinion and not on evidence from randomized trials.
Systematic reviews, including the Cochrane Review “Oral paracetamol (acetaminophen) for cancer pain" by Wiffen et al (2017), point out the lack of evidence of paracetamol's analgesic efficacy. Despite this, the prescribing of paracetamol in conjunction with strong opioids for patients with cancer pain is common practice in most countries worldwide and still recommended by the WHO.
There is a need to establish high quality evidence on whether paracetamol provides additional analgesic effect in cancer pain patients receiving strong opioids. Therefore, a definitive withdrawal study of paracetamol in patients using strong opioids for cancer pain will be an important contribution to provide evidence based care for patients with advanced cancer and reduce patients' burden from possible futile and inefficient treatment practices.
The primary study objective is to establish whether the analgesic efficacy of strong opioids is non-inferior after withdrawal of paracetamol compared to the analgesic efficacy of strong opioids and paracetamol for cancer-related pain.
Outcomes
The primary outcome is average pain intensity at day 8 measured by “Average pain past 24 hours" (numeric rating scale, NRS, 0-10). Secondary outcomes are changes in opioid requirements, opioid related side effects, and patient self-reported rating of overall improvement of pain.
Methods
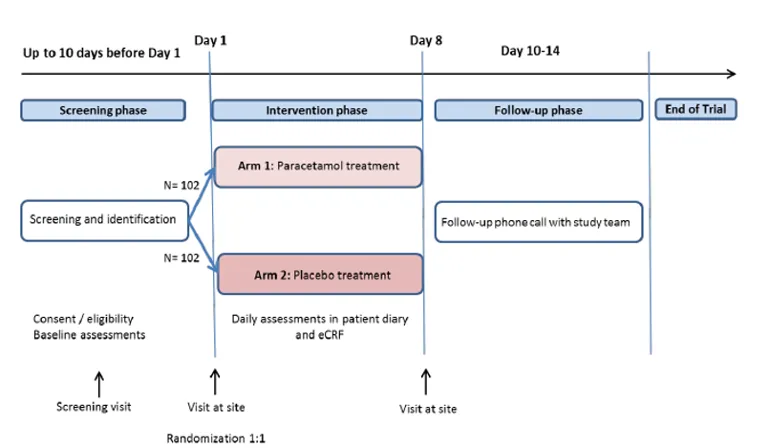
This is a prospective international multi-center parallel group, randomized, placebo-controlled, double-blinded non-inferiority withdrawal trial of placebo versus paracetamol in patients using strong opioids for cancer pain. The study will be conducted at 11 sites in Norway, UK and Italy. The inclusion period is estimated to about 24 months with last patient last visit in Q4 2023. A total number of 204 patients will be included.
Eligible patients have metastatic cancer with a life expectancy of more than 2 months; using both strong opioids and 1 gram of paracetamol 3-4 times daily. When entering the trial at baseline, Day 1, they will be randomized to receive either paracetamol or placebo for seven days in addition to their usual opioid doses. The study team will provide paracetamol or placebo tablets from day 1 of study. After a week, the participants will come to the last study visit (day 8). A follow-up phone call will be conducted 3-7 days after the day 8 visit.
Results
First results are anticipated early 2024.
Main contact: Ørnulf Paulsen